Accentuate the positive: an exciting new psychotherapy development
Last updated on 5th February 2020
"You've got to accentuate the positive. Eliminate the negative. Latch onto the affirmative. Don't mess with Mr In-Between". Bing Crosby sings!
I was really intrigued by the recent paper from Michelle Craske, Alicia Meuret & colleagues - "Positive affect treatment for depression and anxiety: a randomized controlled trial for a core feature of anhedonia" - with its abstract reading "Objective: Loss of pleasure or interest in activities (i.e., anhedonia) is a risk factor for suicidality, treatment nonresponse, and relapse. Extant treatments that focus on reducing negative affect have limited effects upon positive affect (a core feature of anhedonia). We investigated whether a novel intervention aimed at increasing reward sensitivity was more efficacious for positive affect than a cognitive-behavior treatment aimed at reducing threat sensitivity, in individuals with clinically severe symptoms of depression or anxiety, and functional impairment. Method: The Treatment for Affective Dimensions trial was offered in a 2-site randomized study at outpatient treatment centers in Los Angeles and Dallas. Ninety-six patients were randomized to 15 weekly, individual sessions of Positive Affect Treatment (PAT) or Negative Affect Treatment (NAT). The primary outcome was improvement in positive affect (Positive and Negative Affect Schedule-Positive) from pretreatment to 6-month follow-up (6MFU). Secondary outcomes were improvements in negative affect (Positive and Negative Affect Schedule-Negative), suicidal ideation, and symptoms (Depression Anxiety Stress Scales). Results: PAT resulted in greater improvements in positive affect, p = .009, d = .52, and higher positive affect at 6MFU, p = .002, d = .67, than NAT. Participants in PAT also reported lower negative affect, p = .033, d = .52, and lower symptoms of depression, p = .035, d = .34, anxiety, p < .018, d = .30, and stress, p = .006, d = .43 at 6MFU. Finally, probability of suicidal ideation at 6MFU was lower in PAT than NAT (1.7% vs. 12.0%), p < .001. Conclusions: Compared to NAT, PAT demonstrated better outcomes (at 6MFU) on positive affect, depression, anxiety, stress, and suicidal ideation, for patients with symptomatic pretreatment levels of these outcomes."
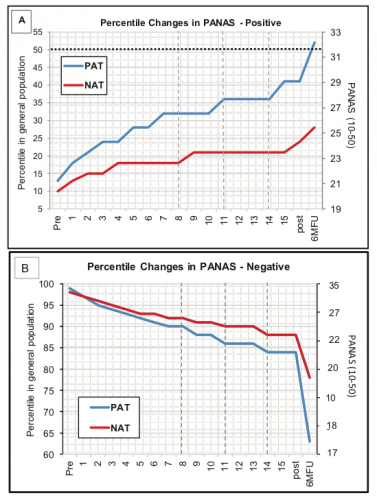
Isn't that interesting ... that a focus on improving positive feelings resulted in greater benefits not only for gains in positive/pleasant feelings but also for reduction in negative/unpleasant feelings than a more traditional CBT approach aimed just at decreasing the negative/unpleasant feelings. This awareness that treatment of depression (and anxiety) might be improved by a greater focus on positive emotion enhancement is pretty widely distributed in the research community. Arnoud Arntz & colleagues from the Netherlands have just published their paper "Positive cognitive behaviour therapy in the treatment of depression: a randomized order within-subjects comparison with traditional cognitive behaviour therapy", while Barney Dunn, Willem Kuyken et al from the UK have produced "Bringing light into darkness: a multiple baseline mixed methods case series evaluation of Augmented Depression Therapy (ADepT)". And in a non-clinical population we even have the loosely related study by Margolis & Lyubomirsky "Experimental manipulation of extraverted and introverted behavior and its effects on well-being". Exciting times ... and all these approaches overlap a fair amount in what they're trying to do. However I think that the Michelle Craske team currently lead the pack. These are their results for changes in positive & negative affect with their Positive (PAT) and Negative Affect Trainings (NAT):
So what do we actually need to do to use these ideas more practically? To explore this, see the next post "Accentuate the positive: how to go about it".